
In this article, we will examine the symptoms caused by SARS Cov2. We will discuss:
1- Behavior and binding to ACE2 receptors
* Steps related to the SARS CoV2 hypercoagulation mechanism, will be marked in red
1- Behavior and binding of SARS-cov2 to ACE2 receptors
- SARS-cov2 binds to ACE2 receptor with the help of Serine protease
Sites where ACE2 receptors are expressed:
ACE2 is abundantly present in humans in the epithelia of the lung and small intestine, which might provide possible routes of entry for the SARS-CoV, however, it is also present on other sites:
– oral and nasal mucosa, nasopharynx
– Lung, especially on lung alveolar epithelial cells
– Stomach
– small intestine, especially on enterocytes
– Colon
– Skin
– lymph nodes
– Thymus
– bone marrow
– Spleen
– Liver
– Kidney
– Brain
– Arterial and venous endothelial cells and arterial smooth muscle cells – This epithelial expression, together with the presence of ACE2 in vascular endothelium, also provides a first step in understanding the pathogenesis of the main SARS disease manifestations.
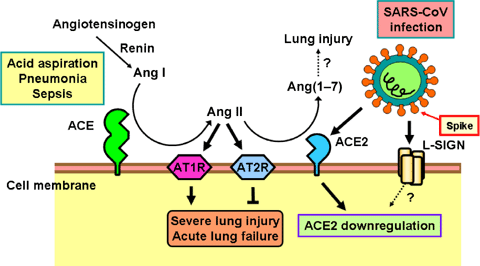
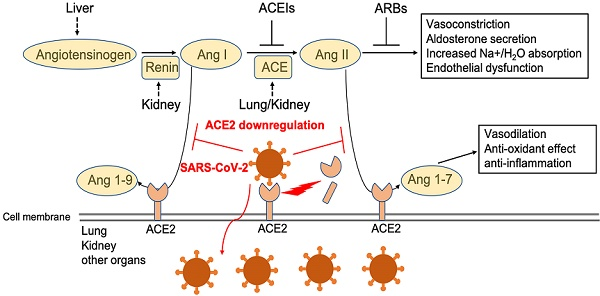
- Effect of ACE2 receptors
- Behavior of AT2 levels theories
In a low level state
Since there isn’t enough AT2 around, it is proposed that Angiotensin Receptor1(ATR1) binds to the catalytic site of ACE2R forming a complex? release of Angiotensin 1,7 ? Activating MAS receptor ? health benefits listed in the diagram (Green box)
– It is believed that ARBS keep the ATR1-ACE2 complex together, leading to the release of Angiotensin 1,7
– ACEi will inhibit the conversion of AT1 ? ATII ? inhibition of Oxidative stress
In a high-level state
– AT2 breaks the ATR1-ACE2 complex, exposing the ACE2 receptor ? SARS COV2 binding, causing:
a. Oxidative stress/activation of NOX
b. Inflammatory response
c. Aldosterone release ? increases in systolic BP
d. Vasoconstriction ? increase in diastolic BP

Cytokine storm and lung damage
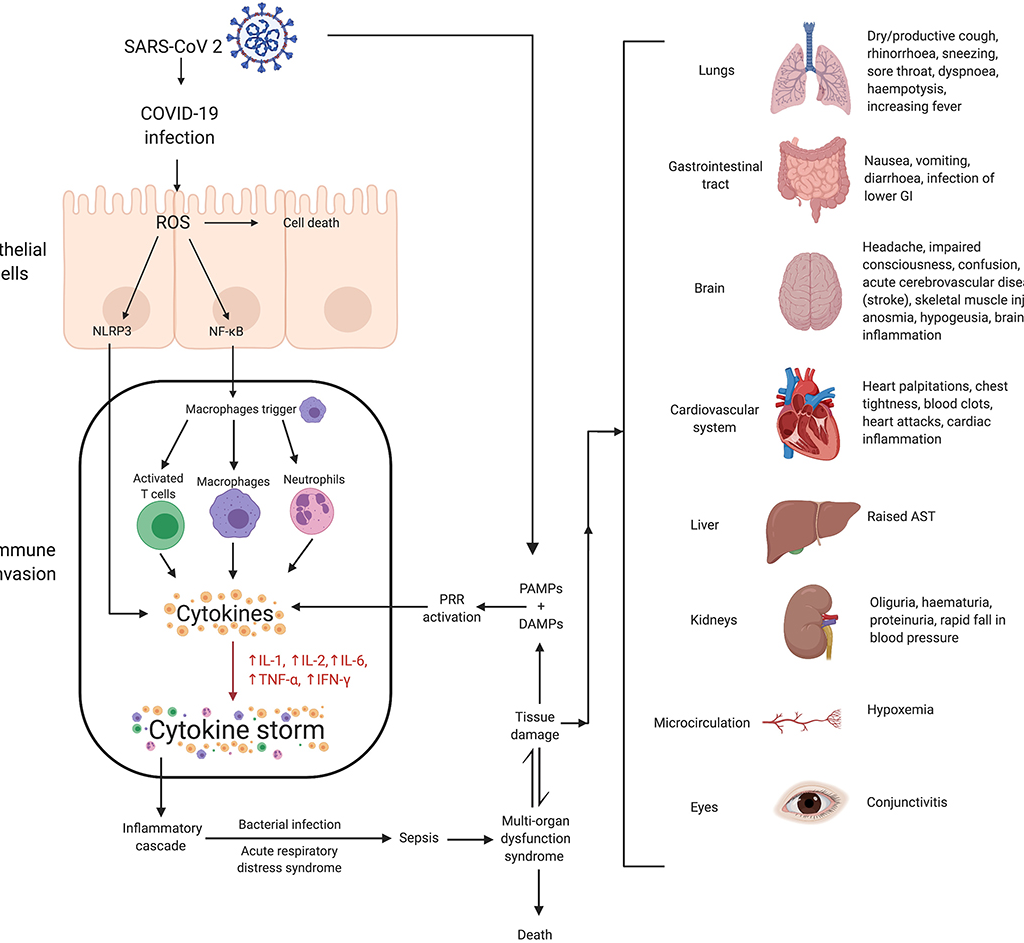
- The cytokine release syndrome (CRS) seems to affect patients with severe conditions.
- Since lymphocytopenia is often seen in severe COVID-19 patients, the CRS caused by SARS-CoV-2 virus has to be mediated by leukocytes other than T cells, as in patients receiving CAR-T therapy; a high WBC-count is common, suggesting it, in association with lymphocytopenia, as a differential diagnostic criterion for COVID-19.
- In any case, blocking IL-6 may be effective.
- Blocking IL-1 and TNF may also benefit patients.
- Although various clinical sites in China have announced the use of mesenchymal stromal/stem cells (MSCs) in severe cases with COVID-19 infection, solid results have yet to be seen. One caveat is that MSCs need to be activated by IFN? to exert their anti-inflammatory effects, which may be absent in severely affected patients as T cells are not well activated by SARS-CoV-2 infection. To enhance effectiveness, one could consider employing the “licensing-approach”: pretreat MSCs with IFN? with/without TNF or IL-1
- Such cytokine-licensed MSCs could be more effective in the suppression of hyperactive immune response and promotion of tissue repair, as licensed-MSCs are effective in LPS-induced acute lung damage .
Lung damage is a major hurdle to recovery in those severe patients. Through producing various growth factors, MSCs may help repair the damaged lung tissue. It is important to mention that various studies have shown that in animal models with bleomycin-induced lung injury, vitamin B3 (niacin or nicotinamide) is highly effective in preventing lung tissue damage It might be a wise approach to supply this food supplement to the COVID-19 patients.
